The rain in eastern Democratic Republic of Congo does not fall; it assaults. It drums against the corrugated tin roofs of Butembo with a deafening, relentless roar, drowning out the sound of human voices. In the valleys, the red volcanic soil turns into a thick, clinging clay that swallows boots and strands vehicles.
But it is not the rain that keeps people awake at night. It is the ledger.
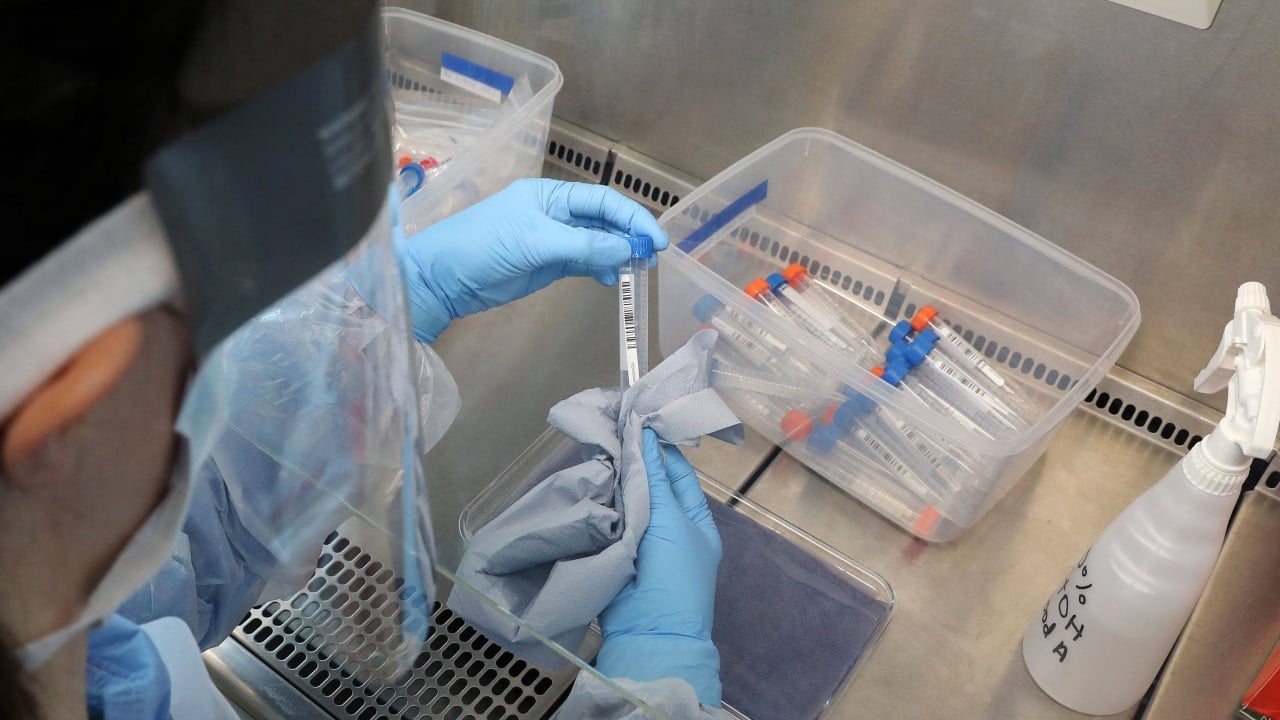
In a small, sterile room shielded by layers of chlorinated plastic sheeting, a black ballpoint pen scratches against a white grid. Another name. Another age. Another cross marked in the column labeled décédé. The numbers have just crossed a terrifying threshold. Nine hundred. Nine hundred souls swallowed by an invisible fire in a region already scarred by decades of conflict.
To the outside world, nine hundred is a data point. It is a headline that flashes briefly on a smartphone screen before being swiped away for something lighter. It is a sterile metric used by bureaucrats in Geneva to allocate funding. But here, nine hundred is a catastrophic tear in the fabric of a community. It is nine hundred empty chairs at dinner tables, nine hundred gardens left untended, nine hundred voices silenced in the dark.
To understand how a virus reaches these heights in the modern era, you have to look past the microscopes and the experimental vaccines. You have to walk down the mud-slicked alleys of North Kivu, where the air smells of charcoal smoke, damp earth, and an underlying, pervasive current of fear.
The Anatomy of Rumor
Consider a woman named Alphonsine. She is a composite of the mothers and grandmothers who hold these hills together, a lens through which we can see the agonizing reality of this crisis.
Alphonsine’s youngest son, Justin, woke up three days ago with a headache that felt like a hot nail driven between his eyes. By evening, the fever arrived, soaking his thin mattress. Then came the vomiting. In a region plagued by malaria and typhoid, a fever is a common thief. You buy some yellow tablets from the market stall, you pray, and you wait.
But this time, the tablets did nothing.
The neighbors whispered through the wooden slats of the walls. They did not whisper about filoviruses or ribonucleic acid. They whispered about the Trésor—the hidden wealth of the hills—and the white trucks of the foreigners.
When the response teams arrive in their pristine white SUVs, wearing heavy goggles and thick rubber suits that make them look like deep-sea divers swimming through the dust, they do not look like healers. They look like astronauts descending into a world they do not understand. They speak French or Swahili with foreign accents. They carry plastic body bags.
"They are stealing our blood," the market vendors say. "They bring the sickness in those bottles to make money from our deaths."
It is easy for someone sitting in a comfortable apartment thousands of miles away to mock these beliefs. It is easy to call them ignorant. But step into Alphonsine’s shoes. For twenty-five years, the only outsiders she has seen are armed militias who burn villages, or corrupt officials who demand bribes at gunpoint. Trust is not a natural resource here; it is a luxury that has been systematically eradicated.
When the men in the spacesuits tell her that she must give up her son, that she cannot touch him, that if he dies, they will bury him in a hole lined with lime without her ever seeing his face again, she does not see medicine. She sees a final, ultimate theft.
So, Alphonsine hides Justin. She pulls the curtains tight. She wipes his brow with a damp cloth, ignoring the dark bruises forming beneath his skin, unaware that every drop of sweat she wipes away is teeming with millions of microscopic killers waiting to jump to her own hands.
This is how nine hundred happens. One hidden bedroom at a time.
The Invisible Stakes
The battle against Ebola is fought on two fronts, and the medical front is actually the simpler of the two. We know how the virus works. It is a clumsy predator, honestly. It cannot float through the air like measles or influenza. It requires intimacy. It demands contact with fluids. In a laboratory, it is easily defeated by soap, bleach, and heat.
The second front is the human mind, and that war is being lost.
The geography of eastern Congo is a labyrinth of shifting allegiances. Dozens of active rebel groups operate in the forests around Beni and Butembo. They strike at night, hacking civilians to death with machetes or firing into crowded market squares. The sound of gunfire is as regular as the evening rain.
Now, place a highly contagious, lethal epidemic into the center of a war zone.
Every time a rebel group attacks a village, the health workers must flee. The contact tracing stops. The thermometers are packed away. The list of people who might have been exposed—the vital map that allows epidemiologists to get ahead of the disease—is broken. The virus uses these violent intermissions to slip into new families, new neighborhoods, new towns.
It is a sinister synergy. The violence feeds the virus, and the virus fuels the panic that breeds more violence. Health centers have been torched. Treatment clinics have come under automatic weapon fire. Investigators have been assassinated in their beds.
Behind the statistics lies a profound structural tragedy. The international community reacts to epidemics like an old fire department. It waits until the house is completely engulfed in flames, then rushes in with sirens blaring, throwing millions of dollars at the smoke. But once the embers are cooled, the trucks drive away, leaving the foundations just as rotten as they were before.
The clinics in eastern Congo do not lack for dedication. The local nurses and doctors are heroes of the highest order, working twelve-hour shifts in stifling heat for wages that are often months in arrears. What they lack are the basics: clean running water, reliable electricity, sterile needles, and gloves. When a hospital lacks gloves, a single undiagnosed patient becomes a biological bomb, transforming the very place meant for healing into a engine of transmission.
The Weight of a Tradition
There is a moment in every culture that is considered sacred: the washing of the dead.
In the villages clinging to the hillsides of North Kivu, when a elder passes, the family gathers. It is an act of profound love and duty. The daughters wash the mother’s hair. The sons dress the father in his finest suit. They touch the skin, they kiss the forehead, they weep over the body, sending the spirit onward with the dignity it deserves.
But a body killed by Ebola is at its most dangerous moment. The viral load is astronomical. The skin is slick with highly infectious fluids.
To the response teams, that body is a biohazard that must be sprayed with chlorine, zipped into double-layered vinyl, and buried immediately by workers wearing thick yellow aprons. To the family, this treatment is an abomination. It means leaving their loved one to wander the afterlife as a restless, dishonored ghost.
The choice the people face is not between science and superstition. It is between physical survival and spiritual survival.
Imagine being told that to save your life, you must desecrate your mother’s memory. Most of us would hesitate. Many of us would choose the ritual over the warning, gambling with the invisible danger to fulfill the visible duty.
One night in a village outside Beni, a traditional healer died. He was a man of immense influence, a keeper of secrets and a fixer of ailments. Hundreds came to his funeral. They touched him. They honored him.
Two weeks later, thirty-two of those mourners were dead. The virus did not care about their grief. It only cared about their proximity.
The Human Ledger
The number nine hundred will soon be nine hundred and fifty. Then a thousand. The curve on the epidemiologist’s chart points stubbornly upward, a black line climbing a mountain of its own making.
But numbers fail us because they flatten the world. They erase the specific texture of suffering. They do not tell you about the five-year-old girl who sat by herself in an isolation ward, watching through a plastic window as her mother died across the room, unable to hold her hand because of the barrier between them. They do not tell you about the young nurse who knew his mask had slipped during a chaotic night shift but kept working anyway, only to feel the first telltale scratch in his throat five days later.
The solution to this crisis will not be found in a faster vaccine rollout or a more advanced isolation pod, though those tools are essential. It will be found when the people in the white suits learn to listen to the people in the mud houses. It will be found when medicine respects the grief of a funeral while protecting the living.
Until that bridge is built, the black ballpoint pen will keep moving across the white grid in Butembo. The rain will continue to lash the tin roofs, washing away the footprints in the red dirt, but leaving the stains beneath the soil completely untouched.